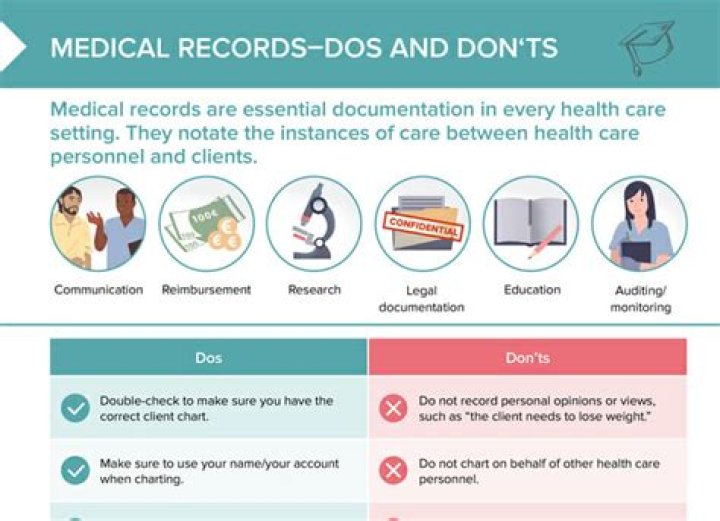
What are 10 standards for documentation in health care records?

Mia Smith
Published Mar 12, 2026
What are 10 standards for documentation in health care records?
Standard 1: Rights.
What records is the health Organisation required to keep?
If you destroy any health records in NSW, VIC or the ACT, you must keep a record of the: name of the person that the medical record related to; time period of the health record (i.e. the date of the first entry through to the date of the last entry); and. date that the record was destroyed.
How long must medical records be kept in Australia?
seven years
The Australian Capital Territory (ACT),3 New South Wales (NSW)4,5 and Victoria6 have legislation which outlines the minimum period of time which medical records should be kept, namely for: an adult – seven years from the date of last entry • a child – until the age of 25 years.
What is included in health record standards?
At a minimum, a medical record must include the patient’s identifying information, including name, date of birth, Social Security number, address, contact information, insurance information, emergency contact information, HIPAA Authorization, and advance directives.
What are the three main types of health records?
Understanding the different types of health information…
- Electronic health record.
- E-prescribing.
- Personal health record.
- Electronic dental records.
- Secure messaging.
Who owns medical records in Australia?
The treatment centre or health professional who creates a medical record owns and maintains the record. However, Australian law considers ownership and access as separate – so although you don’t own the medical record, you can request access to it.
What is health record documentation?
Documentation communicates the what, why, and how of clinical care delivered to patients. These records allow other clinicians to understand the patient’s history so they can continue to provide the best possible treatment for each individual.
How far back to medical records go?
How far back do medical records have to be kept? NSW medical practitioners are required to retain patients’ records for at least seven years from the date of the last entry. If a patient was younger than 18 at the date of the last entry, the records must be kept until the patient turns 25.
How long should health records be retained?
Regulations & Record Retention Federal law mandates that a provider keep and retain each record for a minimum of seven years from the date of last service to the patient.
What are the five C’s in medical record documentation?
Client’s Words, Clarity, Completeness, Conciseness, Chronological Order and Confidentiality.
What is not included in a legal health record?
Equally as important, organizations need to identify information that is not in the legal health record or designated record set. Data such as audit trails, metadata, and psychotherapy notes are not included in the definitions for these record sets.